Approximately 15 in 100,000 people suffer from trigeminal neuralgia (TN) according to western literature. The prevalence in India is not known. If one includes all the different types of trigeminal nerve distribution pain conditions and the undiagnosed cases the prevalence will be much higher. There are several other similar painful conditions. Trigeminal neuropathy, painful traumatic trigeminal neuropathy, traumatically induced neuralgias and atypical odontalgia have many similar features and may represent forms of neuropathic pain. Atypical facial pain, also called persistent idiopathic facial pain has a similar distribution and character of pain.
Symptoms
The International Headache Society has defined TN as a unilateral disorder characterized by brief electric shock-like pains, abrupt in onset and termination, and limited to the distribution of one or more divisions of the trigeminal nerve. The distribution of pain is depicted in the figure. TN is one of the most painful conditions treated by neurologists.
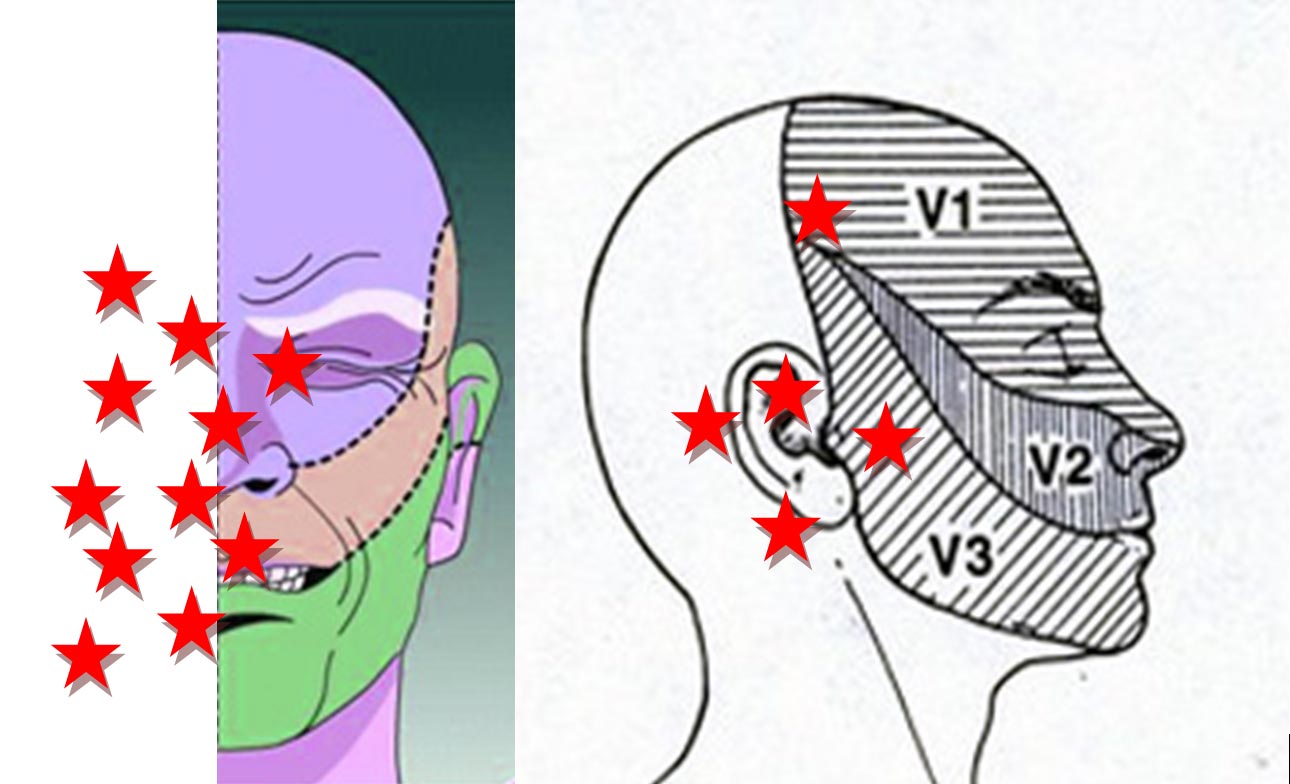
TN generally affects the second and third division of trigeminal nerve, affecting the cheek or chin. The typical attack lasts for few seconds.but may present in clustersof variable severity and duration lasting for few minutes. In between attacks the patient is generally painfree but a background pain may persist in some patients.
It is important to note that pain in this distribution could be because of several conditions listed in the table. The absence of clinically evidence neurological deficit is necessary for the diagnosis of TN. Thus, TN can be idiopathic (due to no known cause) or symptomatic (due to cause). An MRI brain to look at the trigeminal nerve is recommended in all cases of pain in the trigeminal distribution.
Etiology of TN
According to current thinking, TN is caused by compression of the trigeminal nerve root entry zone by a tortuous or abnormal blood vessel (neurovascular compression) leading to demyelination. This leads to hyper excitability of the nerve and central facilitation. Thus, central and peripheral mechanisms may be at work.
Table 1. Differential diagnosis of trigeminal neuralgia
Trigeminal compression – tumors like meningioma, schwannoma, cyst etc
Tolosa-Hunt syndrome
Disorders of jaw, teeth and related structures
Temporomandibular joint dysfunction/arthritis
Sinusitis
Glaucoma
Other cranial neuralgias
Trigeminal autonomic cephalalgias
Cluster headache
Paroxysmal hemicranias
SUNCT/SUNA
Central post stroke pain
Multiple sclerosis
Medical treatment
Generally medical treatment is advised in all patients of TN, with surgical option in patients who are medically refractory.
First line medications
Carbamazepine, oxcarbazepine, pregabalin, gabapentin are the medications used as first line therapy.
Second line medications
Baclofen, lamotrigine, pimozide, lacosamide are second line medications
Other medications
Newer antiepileptic medications like pregabalin and gabapentin are well tolerated and have few interactions. Others like clonazepam, clobazam, phenytoin, topiramate, valproate and tocainide are also tried.
Surgical treatment
Currently in medically refractory cases percutaneous procedures on gasserian ganglion (radiofrequency thermocoagulation, glycerol rhizolysis), gamma knife surgery and microvascular decompression are considered.
These therapies are available at few centers and are successful in the hands of experts. Recurrence can be there after few years. Cost and availability of expertise remain an issue in our country.
Patient's Education
- Epilepsy
- Parkinson Disease
- Migraine
- Stroke
- Bell facial palsy
- Tension type headache
- Alzheimer dementia
- Vertigo
- Neurocysticercosis
- Cerebral venous sinus thrombosis
- Motor neuron disease
- Myasthenia gravis
- Carpal tunnel syndrome
- Wilson disease
- Meningitis
- Febrile Seizures
- Medication overuse headache
- Back pain
- Demyelination and Multiple Sclerosis
- Facial pain
- Neck Pain
- Trigeminal Neuralgia